
Meniere’s disease isn’t just dizziness. It’s a full-body shock to your balance, hearing, and daily life. One minute you’re fine, the next you’re gripping the kitchen counter as the room spins, your ear feels stuffed, and a high-pitched ring fills your head. This isn’t a one-time glitch-it’s a chronic condition driven by something hidden inside your inner ear: too much fluid. And understanding that fluid is the key to taking back control.
What’s Really Going on Inside Your Ear?
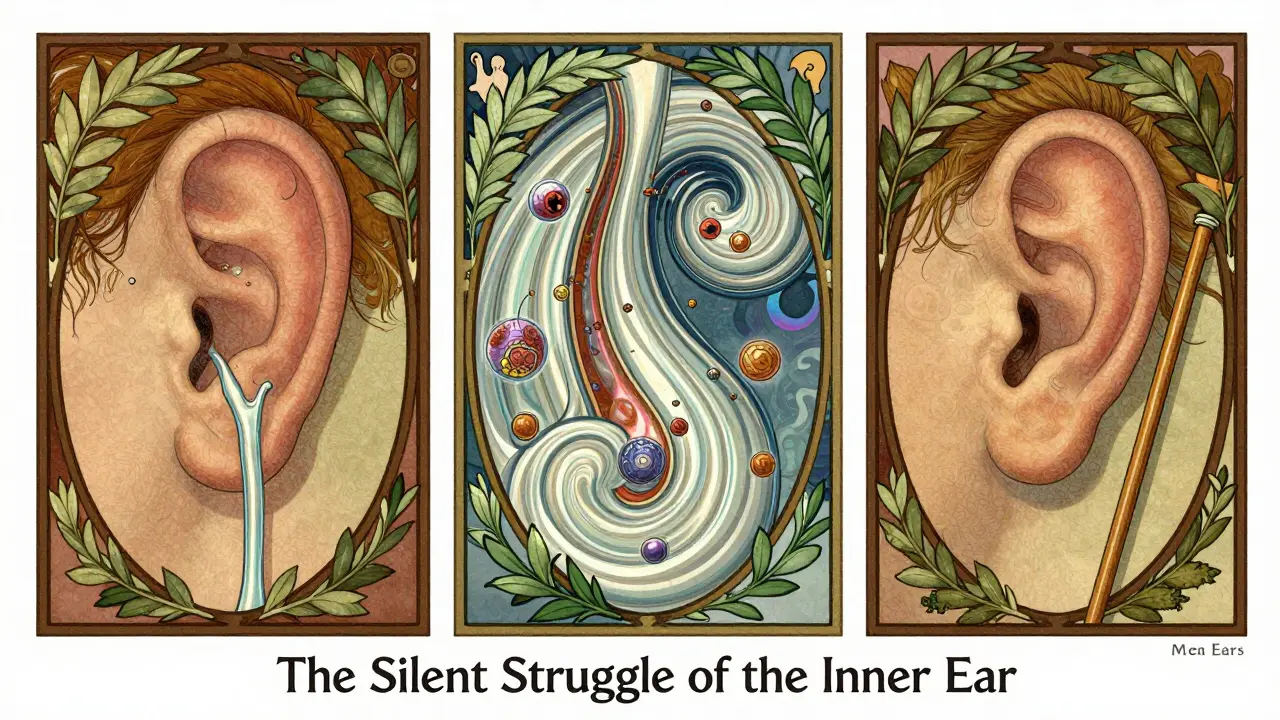
Your inner ear isn’t just a hearing organ. It’s a complex system of fluid-filled chambers that also controls your balance. Two fluids move through it: one is rich in potassium (endolymph), the other in sodium (perilymph). They’re like two different kinds of batteries powering your senses. When endolymph builds up too much-what doctors call endolymphatic hydrops-it stretches the membranes, bursts pressure, and scrambles the signals sent to your brain. That’s when vertigo, hearing loss, and tinnitus strike.This isn’t just theoretical. In 2022, researchers used 3D imaging to map the inner ear in living patients for the first time. They found that in Meniere’s, the saccule (a tiny sac near the cochlea) swells to nearly double its normal size. The utricle? Often still normal. Why? Because its membrane is thicker-12.5 micrometers on average-while the saccule’s is only 8.2. Thinner walls stretch easier. That’s why hearing loss and ringing come first. Vertigo comes later, when the pressure finally pushes into the balance canals.
Why Does the Fluid Build Up?
For over 160 years, doctors have debated the cause. The old theory-fluid overproduction-turns out to be only part of the story. New research shows it’s more about drainage.The endolymphatic sac, a small pouch at the back of the inner ear, is supposed to drain excess fluid. But in 78% of severe Meniere’s cases, this sac’s duct is narrower than 0.3mm. Normal? 0.5mm to 0.8mm. It’s like a clogged kitchen sink. Even if the faucet (fluid production) is turned down, water still backs up.
And it’s not just plumbing. Your immune system is involved too. A 2025 study found that immune cells in the inner ear pump out 4 to 5 times more inflammatory chemicals-like IL-17 and TNF-alpha-in Meniere’s patients than in healthy people. These chemicals weaken the blood-labyrinth barrier, letting in more immune cells, causing swelling, and damaging the delicate hair cells that turn sound into nerve signals. This explains why some people lose hearing even when their vertigo is under control.
Genetics also play a role. About 12% of families with Meniere’s carry mutations in the SLC26A4 gene, which helps regulate fluid movement. And if you’ve had a viral ear infection, autoimmune disorder, or poor circulation in the inner ear, your risk goes up. Most people don’t have one clear cause-they have a mix.
How Do You Know It’s Meniere’s?
There’s no single test. Diagnosis is based on symptoms and ruling out other conditions. You likely have Meniere’s if you’ve had:- At least two episodes of spinning vertigo lasting 20 minutes to 12 hours
- Hearing loss that comes and goes (usually in one ear)
- Ringing or roaring in the ear
- A feeling of fullness or pressure in the ear
And here’s something many don’t know: after 10 or more years, vertigo attacks often stop. That sounds good-but it’s not. It means the inner ear is so swollen and damaged that it’s basically “full.” The pressure doesn’t build anymore because there’s no room left. But now, you’re left with permanent hearing loss, constant imbalance, and trouble walking on uneven ground. That’s why catching it early matters.

What Can You Actually Do to Manage It?
Treatment isn’t one-size-fits-all. It’s layered. The best results come from combining approaches.1. Cut the Salt
It sounds simple, but salt restriction is the most proven first step. The inner ear’s fluid production works like your kidneys. Too much sodium? More fluid builds up. Studies show cutting sodium to 1,500-2,000 mg per day reduces endolymph volume by 23-37%. That’s not just a suggestion-it’s medical therapy. Avoid processed foods, canned soups, and restaurant meals. Read labels. A single slice of bread can have 200mg. You’re not on a diet-you’re protecting your hearing.
2. Diuretics
If diet alone isn’t enough, doctors often prescribe diuretics like hydrochlorothiazide. These help your body flush out extra fluid. They work in 55-60% of people. But they’re not magic. Some people don’t respond because their drainage system is too damaged. Side effects? Dizziness, low potassium, dry mouth. Talk to your doctor about monitoring.
3. Steroid Injections
For sudden, severe vertigo attacks, an injection of corticosteroid (like methylprednisolone) into the middle ear can calm inflammation and improve fluid flow. It’s done in a clinic, takes 10 minutes, and works in 68-75% of cases. Unlike gentamicin (which destroys balance cells), steroids don’t risk more hearing loss. Many people get 2-3 injections over a few months and see big improvements.
4. Emerging Treatments: Targeting Inflammation
Big news in 2025: a new class of drugs called anti-IL-17 monoclonal antibodies showed promise in early trials. They reduced vertigo attacks by 63% and slowed hearing loss by 41%. These are still in testing, but they prove one thing: Meniere’s isn’t just a fluid problem. It’s an immune problem too. Future treatment may involve blood tests to check for inflammation markers before choosing therapy.
5. Surgery (Last Resort)
For the 1 in 5 who don’t respond to anything else, surgery options exist. Endolymphatic sac decompression opens up the drainage pathway. It helps vertigo in 60-70% of cases, but rarely improves hearing. Gentamicin injections, which destroy part of the balance system, stop vertigo in 85-92% of cases-but they can make hearing worse. It’s a trade-off: trade dizziness for partial deafness. Only consider this if vertigo is disabling your life.
What Doesn’t Work
Many people try supplements, acupuncture, or herbal remedies. Some report feeling better, but there’s no solid proof they change the underlying fluid buildup. Avoid unproven “cures.” Focus on what the science backs: sodium control, diuretics, steroids, and emerging immune therapies.
Long-Term Outlook
Meniere’s is progressive. After 15 years, 93% of people have permanent hearing loss in the affected ear. But here’s the hopeful part: the right mix of treatments can slow it down. A 2023 study from the Mayo Clinic found that combining sodium restriction, diuretics, and anti-inflammatory care led to 78% symptom control-far better than any single treatment. And early detection? New 3D imaging can spot fluid buildup before symptoms even start. That means future patients might get treatment before they ever have a vertigo attack.
Living With It
Meniere’s doesn’t define you. Many people manage it well. Keep a symptom diary: note when attacks happen, what you ate, stress levels, sleep. Patterns emerge. Avoid caffeine, alcohol, and smoking-they worsen fluid retention. Stay active, but avoid sudden head movements. Use a cane if you’re unsteady. Tell your family and coworkers what’s happening. You’re not crazy. You’re not imagining it. There’s a real, measurable reason your world is spinning.
Can Meniere’s disease go away on its own?
No, Meniere’s doesn’t go away on its own. While vertigo attacks may decrease over time, this usually means the inner ear is permanently damaged and no longer able to build up pressure. Hearing loss and imbalance often get worse. Treatment doesn’t cure it, but it can slow progression and control symptoms.
Is Meniere’s disease hereditary?
About 10-15% of cases run in families, often linked to mutations in the SLC26A4 gene, which affects fluid regulation in the inner ear. If close relatives have Meniere’s, your risk is higher-but it doesn’t mean you’ll definitely get it. Environmental triggers like stress, salt, or infections often play a role too.
Can stress trigger Meniere’s attacks?
Yes. Stress doesn’t cause Meniere’s, but it can trigger attacks by increasing fluid retention and inflammation. Cortisol, the stress hormone, affects kidney function and inner ear pressure. Managing stress through sleep, exercise, or mindfulness can reduce attack frequency.
Why do some people with Meniere’s lose hearing but not get vertigo?
This is called “vestibular Meniere’s” and accounts for about 18% of cases. In these people, the fluid buildup mainly affects the cochlea (hearing) without triggering the balance canals. They get hearing loss and tinnitus but rarely spin. It’s often misdiagnosed as regular hearing loss until more symptoms appear.
Are there any new treatments on the horizon?
Yes. The most promising is anti-IL-17 therapy, which targets the immune system’s role in Meniere’s. Early trials show it cuts vertigo by 63% and slows hearing loss. Researchers are also testing gene therapies and implantable devices that monitor inner ear pressure in real time. These aren’t available yet, but clinical trials are underway in the UK and US.
Next Steps
If you suspect you have Meniere’s, see an ENT specialist who works with inner ear disorders-not just any audiologist. Ask for a full hearing test, balance evaluation, and possibly an MRI to rule out other causes. Start tracking your salt intake. Keep a symptom log. Don’t wait for a major attack. Early action can preserve your hearing and keep you from being trapped by dizziness.



Kal Lambert
March 18, 2026 AT 02:03Diuretics helped too. Hydrochlorothiazide isn't glamorous but it's real.
Ayan Khan
March 18, 2026 AT 13:26Emily Hager
March 18, 2026 AT 16:41Kal Lambert
March 20, 2026 AT 06:06Melissa Stansbury
March 21, 2026 AT 13:11cara s
March 22, 2026 AT 13:17Shameer Ahammad
March 24, 2026 AT 09:16Amadi Kenneth
March 25, 2026 AT 21:41Alexander Pitt
March 26, 2026 AT 20:43jared baker
March 27, 2026 AT 18:38Manish Singh
March 28, 2026 AT 01:28Michelle Jackson
March 28, 2026 AT 19:40Paul Ratliff
March 30, 2026 AT 16:25SNEHA GUPTA
April 1, 2026 AT 10:11Robin Hall
April 1, 2026 AT 20:06